Clinical research trials are expensive to conduct and continue to rise in cost. Studies by Tufts and JAMA in recent years calculate the average cost to bring a drug to market steadily increasing to more than a billion U.S. dollars1. These rising research costs restrict R&D budgets for drug and device manufacturers, limiting the investments that can be made in new treatments for patients. As the industry continues to adopt decentralized clinical trial (DCT) approaches, there is an opportunity to counteract some of these rising research costs and allow manufacturers to invest in a broader range of life-changing therapies.
Clinical research trials are expensive to conduct and continue to rise in cost. Studies by Tufts and JAMA in recent years calculate the average cost to bring a drug to market steadily increasing to more than a billion U.S. dollars1. These rising research costs restrict R&D budgets for drug and device manufacturers, limiting the investments that can be made in new treatments for patients. As the industry continues to adopt decentralized clinical trial (DCT) approaches, there is an opportunity to counteract some of these rising research costs and allow manufacturers to invest in a broader range of life-changing therapies.
Breaking Down the Numbers
Some of the largest contributors to research expenses include:
Study start-up
Patient recruitment
Total assessments per in-clinic visit
Source data verification (SDV)
Remote and/or onsite monitoring
Participant discontinuation (dropouts)
DCTs can make each of these operational areas more efficient, and therefore reduce the cost of research. It is important to note that these financial benefits may not be realized immediately when conducting an organization’s first DCT. The majority of our customers begin to realize efficiencies post their initial project(s) and after foundational decisions on their preferred DCT designs are established.
Industrywide data and publications on DCT cost savings are also limited at this time. In conducting hundreds of decentralized studies, we have collected and begun to publish the results we have supported2. As the industry conducts more DCTs and contributes to this cost efficiency discussion, we expect more prevalent evidence to offer additional insights. In order to focus on key cost drivers with evidence available today, let’s focus on where DCT approaches can support efficiency specifically with participant recruitment, retention and data quality.
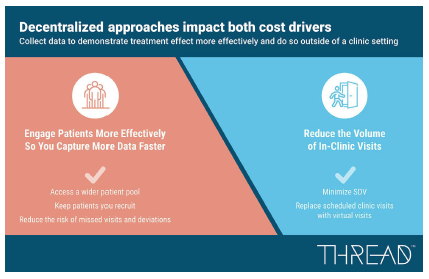
Finding and Engaging Participants
Recruitment is typically a major cost driver (and reason for delays) in clinical trials, typically consuming upwards of 40% of an average clinical trial budget3. With all the advances in digital recruitment models, 90% of recruitment timelines are often doubled post study launch to achieve enrollment targets3. These delays can add millions of dollars of unanticipated costs to the trial. Clinical trial budgets also often assume an average attrition rate of 30% of participants for traditionally designed trials3.
These study designs typically rely on recruitment within a fixed distance around a clinical research site (i.e. 35 mile radius around a site). This assumption is made because the clinical trial visits require all assessments to be completed at the clinic per the protocol’s schedule of events. DCT designs can enable a study to expand the geographic footprint it recruits from (i.e. 200-mile radius around a site) when a hybrid decentralized approach is utilized.
 This approach offers sponsors, sites, and participants a mix of visit options, including telehealth virtual visits, mobile-supported assessments (i.e. ePRO), sensor data collection (i.e. medical devices, wearables), call-center driven data capture, and/or home health visits. By reducing the number of visits that require taking significant time off work, travel, and long clinic visit durations, the commitment for participation can be less burdensome for the patient. In our participant insight projects, this benefit from a DCT design is often noted by potential patients as a big reason they would consider enrolling in a study.
This approach offers sponsors, sites, and participants a mix of visit options, including telehealth virtual visits, mobile-supported assessments (i.e. ePRO), sensor data collection (i.e. medical devices, wearables), call-center driven data capture, and/or home health visits. By reducing the number of visits that require taking significant time off work, travel, and long clinic visit durations, the commitment for participation can be less burdensome for the patient. In our participant insight projects, this benefit from a DCT design is often noted by potential patients as a big reason they would consider enrolling in a study.
To most effectively expand the geographic footprint for trial recruitment, supplemental digital recruitment strategies should be introduced to locate potential participants outside of the site’s databases and refer those participants to the research study. The ability to efficiently support a participant from digital advertisement to study education to opt-in to screening to consent, using a mix of participant website, mobile app, and/or telehealth virtual visits can make a complex onboarding process more simple, transparent, and remote when done correctly. This process can also utilize technology to reduce the costs associated with manual reviews, all on-site pre-screening, etc.
Taking a decentralized approach to recruitment can also support more inclusive studies that encompass more diverse populations. People from geographies far away from trial sites, those with complex work schedules and those reliant on caregivers for transportation are able to participant in trials since interactions can be completed while the participant is at home.
After a participant is recruited into a clinical trial that has adopted a DCT design, the approach continues to offer potential cost reductions with boosted engagement via various support tools, remote data capture, and the mix of visit options available that are not all primarily conducted at the study site. This can lead to higher retention and fewer discontinuations. A recent THREAD report, in partnership with Lokavant, provided evidence that DCTs outperformed industry benchmarks in patient recruitment and retention, when compared with 1,300 traditionally designed studies in 20202.
With more than 70% of trial participants living two-plus hours away from a study center4 and 73% stating that hybrid/decentralized approaches are more appealing5, investing in DCT approaches is an optimal way to reduce common recruitment and retention difficulties that add unexpected costs and generate delays.
Reducing the Cost of Data Capture
Costs associated with protocol required assessments and in-clinic visits represent another area for potential efficiencies. In-clinic visit costs can be broken down into three sections:
1. administration costs
2. site monitoring costs
3. clinical procedure costs
Administration Costs
Administration costs expenses incurred to conduct any site visit such as time of admin staff, time of clinical staff, fixed costs for the location, etc. These costs increase as the number of sites in the trial increase and expand further as the number of enrolled participants increases. Depending on many factors, administration costs can contribute 11% to 29% of clinical trial costs6.
Decentralized approaches leveraging DCT platforms can introduce efficiencies associated with administration costs. The ability for specific visits to be completed as telehealth virtual visits can eliminate some of the administration costs that result with in-person visits. Technology solutions within DCTs such as manual scheduling, appointment reminders, check-ins, check-outs, and other interactions can be conducted via automated activities, limiting resources needed.
Site Monitoring Costs
Site monitoring costs also directly correlate with the number of site visits. In a traditionally designed trial, most or all data is collected at sites and by site staff. As a result, study monitors (i.e. CRAs) are required to visit sites for source data verification (SDV) to ensure the data within the case report form aligns to the original source of information. Even with remote monitoring options, the time and effort required from study teams to monitor data contributes significantly to trial costs, 9% to 14% on average6.
Monitoring and data review costs are reduced with DCT platforms via the removal of data entry that requires SDV such as direct data capture (i.e. ePRO, sensors, etc.) and eSource entry directly into data capture forms by sites and home health nurses. Advanced DCT platforms offer the ability to leverage provisioned and/or bring your own device (BYOD) models for participants, sites and other study team members to enter data directly into the data capture system. These approaches on DCTs provide an opportunity to reduce the amount of data that requires SDV, reducing the overall cost of data monitoring.
Clinical Procedural Costs
Clinical procedural costs factor heavily into traditionally designed study costs. Sites typically negotiate costs for all procedures required for site visits in a trial, which are invoiced to sponsors and/or CROs upon completion. Since all procedures are completed in-person, they also contribute to the total costs, between 15% to 22% overall6.
Procedural costs can be reduced slightly when utilizing hybrid decentralized approaches. Although some of the procedures may be conducted outside of the clinic, the costs associated with them still exist in DCTs. The pricing of some procedures may change when captured via direct data capture models with participants. Overall, this is one cost area that can be minimally impacted and support ensuring that research sites have ample budget per participant to support their business model within a decentralized clinical trial approach.
The combination of cost savings from each of these areas can amount to potential clinical trial savings of 5% to 30% or more at scale depending on the specific DCT strategies that are implemented. For instance, in large, global studies, revising a single in-clinic visit to a telehealth virtual visit can save $1 million or more per protocol6. Using decentralized approaches offers opportunities to reduce and, in some cases, remove high-cost areas.
Conclusion
Decentralized clinical trials provide an opportunity to change how research studies are conducted. They offer a range of benefits such as making studies more flexible, inclusive, convenient, participant-friendly, omni-channel and more for participants and sites. DCTs also offer financial benefits at scaled use depending on which of the efficiency approaches are utilized.
These financial benefits are not the focus of DCTs for most organizations today but are important as our industry defines how decentralized designs will contribute to study efficiencies in the next era of clinical research.(PV)
References: 1https://jamanetwork.com/journals/jama/article-abstract/2762311; 2https://dct.threadresearch.com/hubfs/Reports/THREAD_Lokavant_Report_V2_25JAN2021.pdf; 3https://www.antidote.me/blog/25-useful-clinical-trial-recruitment-statistics-for-better-results; 4https://www.biopharmadive.com/spons/decentralized-clinical-trials-are-we-ready-to-make-the-leap/546591/; 5https://www.ciscrp.org/wp-content/uploads/2019/12/Engagement-Preferences-04DEC.pdf; 6https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7295430/
THREAD is a provider of a proprietary, decentralized research platform and suite of supporting services used by biopharma, CROs, and life-sciences organizations to remotely capture data from participants and sites during, in-between, and in lieu of in-clinic visits.
For more information, visit THREADresearch.com.