 Suppose there’s a problem with your car’s suspension, you pull up to a service station, and the mechanic starts talking about replacing the engine and wheels. The scenario sounds comical, but it captures what could happen if a hasty, soup-to-nuts research approach is misapplied to decentralized clinical trials
Suppose there’s a problem with your car’s suspension, you pull up to a service station, and the mechanic starts talking about replacing the engine and wheels. The scenario sounds comical, but it captures what could happen if a hasty, soup-to-nuts research approach is misapplied to decentralized clinical trials  (DCTs). In this fast-growing area, where research is migrating from trial sites into patients’ homes, the solution is never a one-size-fits-all one.
(DCTs). In this fast-growing area, where research is migrating from trial sites into patients’ homes, the solution is never a one-size-fits-all one.
COVID-19 has been a catalyst for technologies that are key infrastructure for DCTs. The pandemic has sped adoption of remote data collection, telehealth, and mobile research technology — from sensors and wearables to complex home monitoring systems. The tools can increase both efficiency and breadth of data capture. They can ease the burden on patients who wish to join studies, expand points of access allowing for greater patient diversity, and improve the likelihood subjects will stay in a trial. In some cases, the technology provides accelerated approaches that can drive value, even if the initial outlay is greater. Recently, decentralized solutions have earned the respect of global regulators eager to keep patients and investigators safe during the pandemic.
But just because technology-enabled DCTs are available, it doesn’t mean a full-throttle approach is appropriate in every setting, or that such DCTs should look the same in each case. Even when patients are severely ill and a home-based protocol seems a natural fit, the approach may not match patients’ preferences — or the sponsor’s budget. These solutions must be applied with different stakeholder needs in mind. In the simplest terms, patients value optionality, trial sites need flexibility, and industry needs data integrity.
Patient Perspective
A sponsor or contract research organization (CRO) may assume, for example, that late-stage cancer patients in a trial will prefer getting medicines at home. Yet, based on surveys and collaborative efforts with patient groups, we may learn that some patients treasure in-person contact with their oncologists and medical staff. Or they just want to get out of the house and enjoy a routine — having lunch, grabbing coffee — that is woven into their regular site visits.
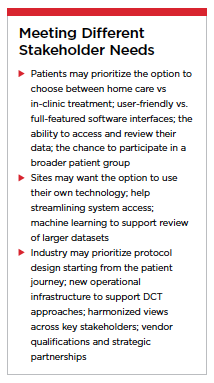 Conversely, there could be an assumption that less-sick patients in a trial for chronic conditions such as type 2 diabetes have greater mobility and won’t mind coming to the trial site. But for any number of reasons — lack of access to transportation, work-related conflicts, or fear of exposure to COVID-19 — the majority may prefer a decentralized approach. The patient also may respond to specific communications related to the study, endorsements by trusted community leaders, lack of an alternative treatment path, or other factors.
Conversely, there could be an assumption that less-sick patients in a trial for chronic conditions such as type 2 diabetes have greater mobility and won’t mind coming to the trial site. But for any number of reasons — lack of access to transportation, work-related conflicts, or fear of exposure to COVID-19 — the majority may prefer a decentralized approach. The patient also may respond to specific communications related to the study, endorsements by trusted community leaders, lack of an alternative treatment path, or other factors.
In each case, it’s the responsibility of trial sponsors and CROs to assess the burdens of the study from a behavioral and patient-journey perspective — that is, by understanding the real-world life experiences of patients and families over the course of the trial and follow-up period. And the learnings will likely be weighed against other scientific and business priorities.
With stakeholder needs converging in some cases but not others, and patient preferences varying from trial to trial, the hunt for one-size-fits-all solutions seems especially precarious. Looking at the latest trends, Goldman Sachs recently predicted that a hybrid approach will dominate. In this model, the demands of patient-centricity “will be further addressed by the availability of both on-site and virtual resources," Goldman wrote, adding that such an approach “is likely to become the new industry standard in coming years."i
Dynamic Assembly
Syneos Health begins the trial design process with a behavioral analysis of site and patient communities reflecting the disease demographics. We collect insights from patients, their families, and advocacy communities when designing each protocol, identifying real-world data sources and endpoints and recruiting subjects. Following an operating philosophy we call Dynamic Assembly, we partner with best-of-breed providers of data assets, digital health technology, and direct-to-patient logistics. We never force-fit owned assets and technology products to purposes for which they weren’t designed.
Instead, both internal and external decentralized capabilities are leveraged to bring the trial closer to patients, but only where it fits the particular case. The process doesn’t start with assumptions that all patients want to be treated at home, or that all sponsors are ready for this approach.
Furthermore, because the enabling technologies behind DCTs are evolving quickly, an effective study strategy draws on talent and resources dispersed through the research community. That’s why Syneos Health partnered with Medable, an innovator in cloud-based DCT, to offer clients a flexible, modular solution that scales to meet the needs of different therapy areas, indications and protocols. We also partnered with Science 37, whose technology platform gives sponsors access to a network of patient communities, telemedicine investigators, mobile nurses, and remote coordinators. The goal is to strengthen both clinical and real-world effectiveness in a fashion most responsive to sponsors’ data-quality needs.
Looking at the larger DCT operating environment, Syneos Health acquired Illingworth Research Group to provide in-home and on-site research nursing services to trials around the globe. This includes mobile research nurse services for patients in their homes that can effectively slash wasted travel time.
Harmonization
The case against one-size-fits-all in decentralized trials in no way cancels the need for industry standards or coordination. While patients and investigators benefit from freedom to mix and match the best technologies, it helps no one if disparate devices can’t communicate, data can’t be ported across institutional or study boundaries, or a cacophony from unsynchronized devices drowns important signals in the data.
Writing in the New England Journal of Medicine, a team at Harvard Medical School and Harvard Business School identified at least three reasons the virtues of remote patient monitoring — a key piece of the DCT toolkit — could be compromised if the sector advances without a commitment to interoperability among devices and the collection of evidence showing patients benefit.ii
In the first place, vendors currently can pursue marketing approval without demonstrating clinical effectiveness in disease management. Secondly, reimbursement through Centers for Medicare & Medicaid services (CMS) is not contingent on meeting a clear set of specifications or standards; Third, the expansion of fee-for-service reimbursement for remote patient management (RPM) services with or without high-quality clinical data incentivizes their use without follow-up or prudent surveillance.
Harmonization efforts by the Decentralized Trials & Research Alliance (DTRA) and other bodies may set the stage for better-orchestrated technology integration as DCTs evolve. No one wishes to stymie innovation through unnecessary regulation or self-imposed constraints. That said, collecting data in a harmonized fashion would allow data to be pooled and all valuable outputs fed into repositories (data lakes) that can be used for meta-analyses, exploring research hypotheses, feasibility testing, and even understand operational consequences of decisions in a study.
In order to create fit-for-purpose DCT solutions that meet multiple stakeholder needs, sponsors and CROs must move forward with flexibility and agility, steering clear of one-size-fits all approaches. Regulators in global markets have signaled an openness to expanded use of decentralized research models — a welcome trend. And industry organizations are helping ensure that initiatives on behalf of patients are harmonious, so the data we generate is meaningful and valuable to all.(PV)
References:
i Virtual Clinical Trails: pandemic accelerating the modernization of clinical trials. April 2021. Godman Sachs Equity Research. Accessed May 6, 2021
ii Mecklai K, et al. 2021. Remote Patient Monitoring—Overdue or Overused? [online] New England Journal of Medicine. Available at: < https://www.nejm.org/doi/full/10.1056/NEJMp2033275>. Accessed May 7, 2021
Syneos Health is the only fully integrated biopharmaceutical solutions organization. The company, including a contract research organization (CRO) and contract commercial organization (CCO), is purpose-built to accelerate customer performance to address modern market realities. We bring together about 25,000 clinical and commercial minds with the ability to support customers in more than 110 countries.
For more information, visit syneoshealth.com.