With advances in genomics sequencing combined with AI and other tools to speed up data analysis, the potential for quickly diagnosing and ultimately developing therapies that can treat patients with rare diseases in real time grows.
The rare diseases space has come on leaps and bounds over the past decade. Advances have been made in DNA sequencing and gene therapy is showing huge potential for addressing several rare diseases. Artificial intelligence is helping to speed up the pace of diagnosis and treatments, and regenerative therapies are demonstrating potential to cure rare genetic conditions.
While these breakthroughs show how far the field has advanced, about 95% of the approximately 6,000 to 8,000 rare diseases still have no approved treatment. Around 80% of rare diseases have an underlying genetic cause and more than half of patients are children. Furthermore, 30% of children with a rare disease 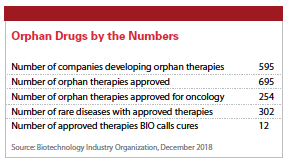 will die before the age of 5. These patients can’t wait the 10 years it typically takes to carry out research and bring products to market.
will die before the age of 5. These patients can’t wait the 10 years it typically takes to carry out research and bring products to market.
The goal for these patients is to develop treatments and cures in real time based on genomics. But what needs to happen to move closer to that objective?
In its report, Imagining the Future of Rare Diseases, Global Genes notes that beyond scientific obstacles, barriers to the breakthroughs patients so desperately need include financial, policy, and man-made issues that result from competing interests. As the report states, success comes from working together toward a common goal.
“From a global perspective, it’s critical that we pool resources in drug discovery and connect patient communities to drive treatments to approval and marketing for everyone, including people living with rare diseases," says Nerissa Kreher, M.D., chief medical officer at Tiburio Therapeutics.
There is a need for tight, coordinated collaboration between key stakeholders, including patients, pharmaceutical/biotechnology companies, researchers, clinical investigators, pathologists, diagnostics companies, academia, and regulators, says Ujwal Pyati, Ph.D., practice leader, scientific strategy, strategy & planning, W2O.
“Rather than adhering to classical clinical trial protocols and approval processes that often take years to complete, regulators must be willing to advance  therapeutics with strong evidence, based on small numbers of patients, and even data from preclinical models to support quick, small-scale studies," Dr. Pyati says.
therapeutics with strong evidence, based on small numbers of patients, and even data from preclinical models to support quick, small-scale studies," Dr. Pyati says.
Sequencing Technology Meets Patient Need
Advances in sequencing technology combined with AI tools that make it possible to analyze huge volumes of data very quickly, mean determining a patient’s genetic disease can now be done within days or weeks, compared with months and years, and at a much lower cost than just a few years ago.
“The incredible investments in full genome sequencing and interpretation have allowed patients or their caregivers to quickly realize whether they are suffering from a monogenetic disorder," says David Fischer, Ph.D., executive director discovery sciences of Scientific Advisory Services at Charles River.
This is important because treatment must begin with diagnosis.
According to Don Gabriel, M.D., Ph.D., senior director, medical oncology and scientific strategy, UBC, diagnosis for the molecular disease is typically made on as little as 20 microliters of blood placed on a filter paper wafer and then analyzed by tandem mass spectroscopy.
“Once the diagnosis is established, further details of the disease are made by whole gene sequencing — WGS — that provides more details of the defect," Dr.  Gabriel explains. “If necessary, the defective gene can be expressed by a variety of different means to yield the defective protein. A comparison of the normal protein and the defective protein can then be analyzed using computational analysis."
Gabriel explains. “If necessary, the defective gene can be expressed by a variety of different means to yield the defective protein. A comparison of the normal protein and the defective protein can then be analyzed using computational analysis."
Such tools allow for the more rapid development of potential drugs, which enables scientists to design and synthesize an effective drug to correct the defect, he continues.
Drug development for rare diseases can be accelerated by integrating clinical, electronic medical records, and other -omics data, says Rama Kondru, Ph.D., chief technology officer and chief information officer at Medidata.
“Data from disease indications, biomarkers, pathways, and patient journey  understanding are critical to positioning therapies for success and bending the development cost curve," he says.
understanding are critical to positioning therapies for success and bending the development cost curve," he says.
Technological advances have made it easy to create the raw materials, such as vectors and editing constructs, that would serve as the basis of a genetic therapy for an individual with a given genetic disorder, says Cynthia Verst, Pharm.D., president, Design and Deliver Innovation, R&D Solutions at IQVIA. What’s not so easy, Ms. Verst says, is converting these materials into true therapies in real time.
“The most feasible model is a platform technology where one delivery system or methodology is used to deliver a specific genetic fix for many different genetic alterations, and only the genetic raw materials need to be changed within the delivery system for each new, unique patient," Ms. Verst says. “This model would require that the given disorder be approachable with the platform delivery system. Different disorders would require delivery of different genetic fixes to specific organs, for example, liver, bone marrow, brain, etc., so a variety of platforms would be needed."
Craig Lipset, founder of Clinical Innovation Partners, says platforms such as the NIH’s All of Us Research Program or Verily’s Project Baseline are valuable ways to share research quality data.
“Patients with a rare disease who are using those platforms can continue to share data on those platforms as they become eligible for investigational new medicines, creating a sustained data source," he says.
Barriers to Real-Time Treatment
According to Gaurav Shah, CEO of Rocket Pharmaceuticals, developing on-demand drugs tailored to a patient’s genetic mutations would require overcoming several clinical and regulatory issues.
 “For these types of treatments to reach their potential, an accommodating FDA approval process is critical," he says. “Theoretically, for these types of approvals to be possible, a company would first have to prove the safety and tolerability of the platform, for example AAV and/or lentiviral vectors and associated materials. Once clinical trials determine the platform itself to be safe, the specific gene of interest could be switched out each time a new patient needs the therapy. This type of plug-and-play approach would make it possible to personalize therapies to the rare patient’s specific mutation."
“For these types of treatments to reach their potential, an accommodating FDA approval process is critical," he says. “Theoretically, for these types of approvals to be possible, a company would first have to prove the safety and tolerability of the platform, for example AAV and/or lentiviral vectors and associated materials. Once clinical trials determine the platform itself to be safe, the specific gene of interest could be switched out each time a new patient needs the therapy. This type of plug-and-play approach would make it possible to personalize therapies to the rare patient’s specific mutation."
For rare disease, it is essential to have a scalable way to characterize the disease — its progression, characteristics, prognosis, and symptoms, says Nancy Yu, CEO of RDMD.
“In other words, how do you run a natural history study to better understand the baseline disease so that industry researchers can design clinical trials and educate FDA to pave a regulatory pathway forward?," she asks.
 “As amazing as it could be, it would take radical advancements in molecular biology, drug delivery, and in vivo gene-editing technologies, as well as possibly a tectonic shift in the U.S. regulatory framework, for real-time drug development for rare disease patients," says David Marks, Ph.D., VP, medical director, Elevate Healthcare.
“As amazing as it could be, it would take radical advancements in molecular biology, drug delivery, and in vivo gene-editing technologies, as well as possibly a tectonic shift in the U.S. regulatory framework, for real-time drug development for rare disease patients," says David Marks, Ph.D., VP, medical director, Elevate Healthcare.
Ms. Verst notes that the concept of a technology platform to treat different genetic alterations has one major challenge: each disorder is unique, which means each one would require initial preclinical research to establish the feasibility of the genomic therapy.
“This is made even more challenging by a lack of relevant model systems and biomarkers for many rare disorders," she says. “Appropriately scaled clinical-genomic datasets will be critically important for elucidating pathobiology and identifying relevant genetic targets within individual disorders."
However, she notes that once preclinical work is accomplished, real-time treatment of patients with that disorder, even ones carrying unique mutations, would be more feasible.
Safety is another issue when it comes to real-time treatment. Ms. Verst says there would need to be enough confidence in the safety of delivery systems to reuse them for different genetic alterations without significant study of safety for each unique therapy.
At a broader level, developing medicines to treat rare diseases presents scientific and operational challenges.
Amy Graham, client engagement officer, Ogilvy Health, says the complex biology of many rare diseases makes it difficult to design and implement a drug development program. The small population of patients with a rare disease makes recruitment for and conducting clinical trials difficult.
“However, the genetic revolution may well be the driver for advancing drug development and care for these patients," she says.
Dr. Marks says treating genetic loss of function is the lowest hanging fruit but while two therapies — Zolgensma and Luxturna — have been approved, both went through traditional regulatory pathways.
 “Considering current technology, any similar gene therapy developed in real time for patients could be less specific and efficacious," he says. “Even real-time treatment for gain-of-function for monogenetic disorders such as Huntington’s disease, where the exact gene and disease course are well understood, would be difficult."
“Considering current technology, any similar gene therapy developed in real time for patients could be less specific and efficacious," he says. “Even real-time treatment for gain-of-function for monogenetic disorders such as Huntington’s disease, where the exact gene and disease course are well understood, would be difficult."
Dr. Marks says first the gene would have to be edited, for example using CRISPR-Cas9, or silenced, and even with gene silencing, there are two competing approaches under development and as yet it’s uncertain which is the most efficacious and safe method.
“Rapid deployment of protein/enzyme replacement therapy is the most likely future candidate for this but there remains the problem of ensuring the replacement protein can actually access the intended targets, and without rigorous testing we could not truly know," Dr. Marks says. “The most likely chance for success in this area would be a comprehensive, high-fidelity plug-and-play platform that allows construction of DNA or protein sequences, packaging into vectors, and targeting engagement verification before deployment."
Real-Time Breakthroughs
While barriers to achieving real-time treatments for rare diseases will need to be overcome to achieve significant advances, the industry is at or approaching the point for some rare diseases.
“Strimvelis, an autologous gene-modified cell therapy for the ultra-rare adenosine deaminase-deficiency form of severe combined immunodeficiency, also known as ADA-SCID, first developed by GlaxoSmithKline, is essentially a real-time, or near real-time, personalized drug made from a patient’s own bone marrow cells by inserting a corrected ADA gene," says Daryl Spinner, Ph.D., managing director, real-world value and strategy, Evidera. “Orchard Therapeutics is continuing to build on that platform for other rare genetic diseases, with therapies in mid-to-late stage clinical development for four separate disease areas.
“Bluebird bio received conditional approval in Europe in June 2019 for Zynteglo, an autologous gene-modified cell therapy for patients with transfusion-dependent beta-thalassemia, which takes a personalized approach to restoring gene function," Dr. Spinner continues. “Some cancer immunotherapies and personalized therapeutic vaccines also provide a model for how personalized drugs could be developed in real time."
Approved immunotherapies like Kymriah and Yescarta for B-cell-based blood cancers are personalized gene-modified cellular therapies created by genetically engineering a patient’s own T-cells to recognize and kill the cancerous B-cells.  There are therapeutic cancer vaccines in clinical development for various solid tumors that are highly personalized drugs that leverage information on the patient’s unique cancer profile at the molecular level to ensure therapeutic effect in that patient. Each cancer vaccine is designed in real time to be effective only for a single cancer patient at a time.
There are therapeutic cancer vaccines in clinical development for various solid tumors that are highly personalized drugs that leverage information on the patient’s unique cancer profile at the molecular level to ensure therapeutic effect in that patient. Each cancer vaccine is designed in real time to be effective only for a single cancer patient at a time.
According to Dr. Fischer, with several drugs on the market, for example oligonucleotide-based drugs (ASO) or gene therapies, it is now conceivable to rationally design candidate drugs and test them in an expedited manner for pharmacodynamic efficacy and preclinical safety.
Dr. Kondru says there is a need to repurpose some existing drugs and clinical candidates based on their biomarker profile to bring about new solutions for rare diseases.
This is starting to happen.
Dr. Pyati describes a recent example where a child’s ultra-rare lymphatic condition was identified by clinicians, diagnosed definitively through genomic sequencing by pathologists, and brought into preclinical testing in the zebrafish model system.
“Researchers were able to introduce the same genetic mutation into zebrafish and screen multiple small molecules to identify which pharmacologic approach could alter the disease phenotype," he says. “Through this approach, a positive hit, already developed by Novartis for a different disease, was identified. This molecule was quickly moved through an approval protocol by the FDA and administered to the child, with tremendous results that were impossible with other available agents."
He notes that in small patient populations with standardized biomarkers and easily interpreted endpoints, the FDA can begin the process to make drug candidates more readily available to patients who so desperately need them.
Dr. Gabriel explains that some treatments involve inserting a normal gene into the patient, a procedure that is usually accomplished by putting the normal gene into a virus and then infusing it into the patients.
“Sometimes the patient’s stem cells are isolated and then transfected with the virus containing the normal gene followed by reinfusing the genetically engineered stem cells back into the patient," he says. “Before being able to  correct a patient’s genetic abnormality, the normal enzyme was infused into the patient to replace the missing or defective protein. This method requires repeated infusions that can be associated with adverse events. With gene therapy, the hope is that repeated infusions can be avoided."
correct a patient’s genetic abnormality, the normal enzyme was infused into the patient to replace the missing or defective protein. This method requires repeated infusions that can be associated with adverse events. With gene therapy, the hope is that repeated infusions can be avoided."
Ms. Graham says gene therapy for rare diseases has achieved remarkable success, resulting in recent market approvals.
“With a robust clinical pipeline, gene therapy is expected to continue to be a driver in providing therapeutic advancements in the treatment of rare diseases," she says. “The next breakthrough may come from genome editing, a process that involves cutting out mutations in DNA and replacing them with new genetic material. This is an exciting idea because if refined to a level that is safe and effective, the prospect of eradicating genetic diseases is a tangible possibility.
 There are several different genetic tools available for genome editing. The CRISPR technique uses the enzyme called CAS9, derived from bacteria, to edit out designated areas of the genome. There is currently a great deal of excitement about CRISPRs, because they are easier to use, can be programmed to act on several regions of the genome at once, and have been shown to be most accurate in identifying and cutting out mutations in DNA."
There are several different genetic tools available for genome editing. The CRISPR technique uses the enzyme called CAS9, derived from bacteria, to edit out designated areas of the genome. There is currently a great deal of excitement about CRISPRs, because they are easier to use, can be programmed to act on several regions of the genome at once, and have been shown to be most accurate in identifying and cutting out mutations in DNA."
Meanwhile, Medidata has partnered with the Castleman Disease Collaborative Network Data (CDCN) to explore how data and analytics can accelerate realization of personalized medicine for life-threatening rare diseases.
“This collaborative study combined patient data with machine learning capabilities to help better understand Idiopathic Multicentric Castleman Disease (iMCD) disease," Dr. Kondru says. “Our product, Medidata Rave Omics is built to discover new patient subgroups and novel biomarkers based on genomic and  proteomic signatures. This product was successfully used to derive personalized biomarkers for Castleman Disease and was a great example of how machine learning technology partnered with data can identify new patient subgroups, accelerate diagnosis, and ultimately, treatment."
proteomic signatures. This product was successfully used to derive personalized biomarkers for Castleman Disease and was a great example of how machine learning technology partnered with data can identify new patient subgroups, accelerate diagnosis, and ultimately, treatment."
For extremely rare, personal mutations causing rapidly progressive disorders, there is a route for expanded access approvals by the FDA that could potentially allow a patient to be treated with a personalized therapy, developed specifically for their mutation.
“We have seen this process applied by Dr. Timothy Yu at Boston Children’s Hospital and Lauren Black, Ph.D., from Charles River with milasen, an intrathecal ASO developed for a patient with a rare form of Batten’s disease," Dr. Fischer says.
Other advances in treatment of rare diseases continue to be made. For example, Tiburio is leveraging pharmacological developments to advance unique chimeric compounds called dopastatins that have the potential to become the first effective pharmaceutical treatment for a rare neuroendocrine disease called nonfunctioning pituitary adenoma.
Carving Out a Path to Move Forward
According to Lori Styles, senior medical director at AbbVie, it would take some sort of merit system, reimbursement program, or compensation to develop treatments in real time for rare disease patients based on their genome affliction.
Dr. Styles says with genome afflictions, pediatrics are top of mind and to develop therapies in real time for rare disease patients, something like pediatric exclusivity should be offered.
“This results in a win-win for patients, the industry, and the FDA," she says. “Essentially, companies can be rewarded for doing good, well-designed studies for pediatrics by providing exclusivity to their therapies."
 According to Evidera’s Dr. Spinner, a combination of advancing basic and clinical science, maturing regulatory processes for gene-based therapies, the increasing number of clinically validated therapeutic gene delivery platforms, ranging from autologous cell-based and viral-based, to nucleic acid-carrier formulations, and “naked" nucleic acid delivery approaches are moving the industry closer to a future reality where more and more personalized drugs for rare genetic diseases will be designed in real time to treat and, in some cases, cure the patient.(PV)
According to Evidera’s Dr. Spinner, a combination of advancing basic and clinical science, maturing regulatory processes for gene-based therapies, the increasing number of clinically validated therapeutic gene delivery platforms, ranging from autologous cell-based and viral-based, to nucleic acid-carrier formulations, and “naked" nucleic acid delivery approaches are moving the industry closer to a future reality where more and more personalized drugs for rare genetic diseases will be designed in real time to treat and, in some cases, cure the patient.(PV)












